MULTIPLE MYELOMA
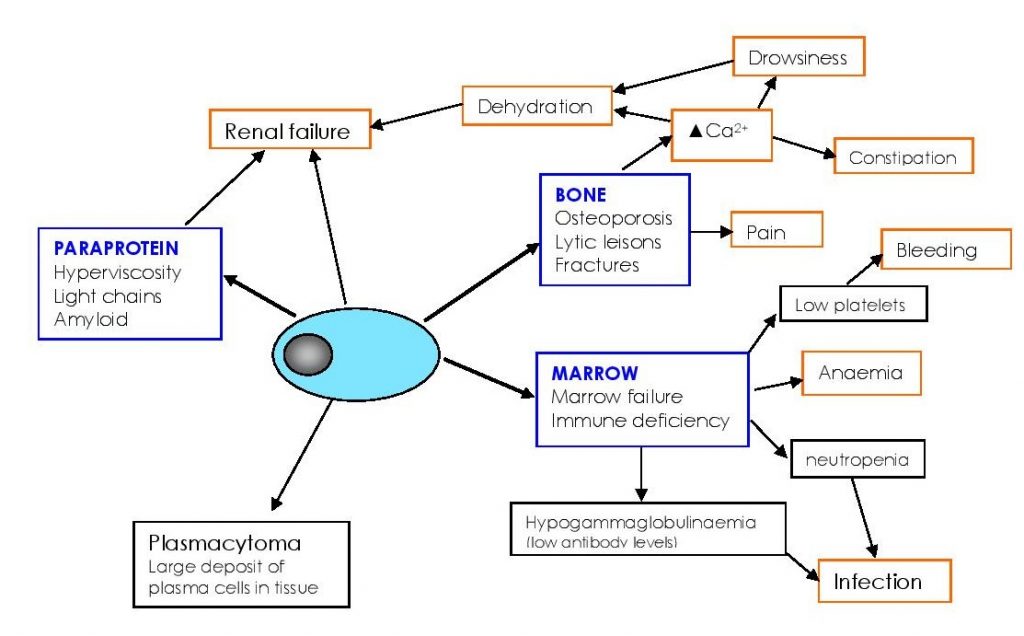
Myeloma is a cancer of the bone marrow plasma cells. The characteristic features are lytic bone lesions (fractures), accumulation of plasma cells and the presence of a paraprotein (monoclonal antibody).
DIAGNOSIS
- The diagnosis relies on a cluster of features; as the individual features may be seen in other disorders
- Paraproteins can be seen in MGUS, lymphoma, Waldenstrom’s macroglobulinaemia, CLL, Primary Amyloid, heavy chain disease, CHAD or less commonly transiently.
- Lytic bone lesions and fractures can be seen in solid tumours invading bone – eg prostate cancer or breast cancer
- Myeloma requires:
- Increased plasma cells in the marrow
- Paraprotein (in serum or urine)
- Bony lesions
TREATMENT
General measures:
- Renal failure requires rehydration and treatment for gout
- Hypercalcaemia (high serum Calcium) requires iv fluids, diuresis, and drugs to reduce the calcium (often biphosphonates – Zoledronic Acid, Clodronate or pamidronate)
- Bone compression of the spine and spinal cord requires urgent neurosurgery, steroids and radiotherapy / chemotherapy
- Bone pain due to lytic lesions often responds to radiotherapy
- Anaemia – transfusion
- Severe recurrent infections – antibiotics, regular immunoglobulin infusions
Chemotherapy:
- The type of therapy will depend on the patient’s age, general health, extent of myeloma and its complications.
- Palliative therapy: This type of treatment is aimed at reducing or preventing the problems associated with myeloma without causing excessive side-effects of treatment. Treatment is not curative but aimed at providing a decent quality of life. Elderly patients with lots of additional medical problems would be best served by this approach.
- Standard chemotherapy: This is used to bring the disease under control, but again without the prospect of cure. Substantial remission and good quality of life is often achieved but the disease becomes active eventually.
- High-dose therapy (Stem cell transplant): This is reserved for younger patients who are fit enough to tolerate the treatment. Even in this group cure is rarely (if ever) achieved, but a long period of good life with the disease being dormant is possible.
Drugs used in Myeloma :
- Proteosome Inhibitors: Bortezomib, carlfilzomib, ixasomib
- Immunomodulatory Drugs (IMIDs): Thalidomide, Lenalidomide, Pomalidomide
- Monoclonal Antibodies: Daratumumab
- Conventional chemotherapy drugs: Melphalan, Cyclophosphamide, and many more
- Steroids: Dexamethasone, Prednisolone
- These drugs are often used in combinations, and when one class of drug fails, another class is used.
Stem cell transplantation is usually performed after 4 cycles of chemotherapy; stem cells are mobilised using high-dose cyclophosphamide and G-CSF; then the myeloablative therapy is high-dose melphalan. See the section on Stem Cell Transplantation.
Outcomes are improving with the improvements in detecting disease, managing the complications of the disease as well as more choice and better drugs to treat the disease.
Traditionally Myeloma was considered a terrible disease with the average life expectancy only 1-2 years. With advances over the last few years, myeloma is now considered a chronic disease, which remains incurable, but often controllable. Drug combinations are used, and when they fail the next drug is used. As we have more effective drugs, the ability to continue therapy improves. Myeloma does remain a very serious disease, with many potential complications. The median life expectancy is 4-6 years. Some live much less, some have the benefit of a much longer course with the disease.